49 year old with vomitings
2 nd August 2022.
A 49 year old male ,auto driver by occupation came with chief complaints of vomitings and loss of appetite.
History of presenting illness:
Patient was apparently assymptomatic 10 years back and then he developed weaknesses and fever for which he went to local hospital and diagnosed to be having diabetes for which he was under medication.And after one year he complained to have head ache and was diagnosed with hypertension, for which he used medication for one year and stopped.6 years back he developed weakness of limbs for which he was found to be having low potassium and was treated accordingly.
25 days ago patient complained of vomitings ( 5 episodes per day ,non bilious and non projectile). Numbness in the left upper limb and lower limb , deviated jaw to the right side , unable to close the left eye for which he was taken to the hospital and diagnosed to have acute ischemic stroke, he was treated accordingly and discharged.after one week he had vomitings ( 6 episodes) and he was taken to the hospital and they were told that he had high blood sugars and he was treated.
Since 3 days he has 6 - 7 episodes of vomitings per day, and he was admitted at our hospital.
Past history:
History of diabetes millitus since 10 years ( Tab met Forman -500 mg),
History of hyperTension since 9 years .
Not a known case of Asthma, tuberculosis,CAD.
Personal history:
Diet:mixed
Appetite: Normal
Sleep : Normal
Bowel and bladder: regular
Addictions:smokes ( 10 cigarettes per day)
Alcohol consumption ( 3 times per week)
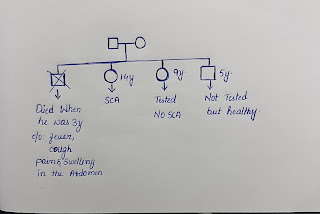
Family history:
No relevant family history.
General examination:
Patient is conscious, coherent but not cooperative
Moderately built and nourished.
Pallor:absent
Icterus:absent
Clubbing:absent
Cyanosis:absent
Generalised lymphadenopathy:absent
Pedal edema :absent
Vitals:
Temperature:98.8
Pulse rate:76
Respiratory rate :20
Blood pressure:
Spo2:98
GRBS:
Systemic examination:
Higher mental functions:
MMSE could not be assessed.
Speech : normal
Behaviour: sluggish
Gait: patient couldn’t walk.
Reflexes:
CVS: s1 s2 heard no murmurs .
Respiratory: bilateral air entry present , normal vesicular breath sounds heard.
Abdomen:
Soft and non tender ,
No hepatomegaly and spleen is not palpable.
Provisional diagnosis:
Diabetic ketoacidosis secondary to poor glycemic control and non compliance to insulin.
Investigations:





Treatment:
Zofer - 4 mg I/v TID
Pan I/v TID
Tab ecospirin -75 mg
Tab Atorvas -90 mg
Tab clopitab
Tab pregabe
Tab sucrolyte
IV fluids .


Comments
Post a Comment